Talk:Tianeptine
| This is the talk page for discussing improvements to the Tianeptine article. This is not a forum for general discussion of the article's subject. |
Article policies
|
| Find medical sources: Source guidelines · PubMed · Cochrane · DOAJ · Gale · OpenMD · ScienceDirect · Springer · Trip · Wiley · TWL |
| This article is rated B-class on Wikipedia's content assessment scale. It is of interest to the following WikiProjects: | |||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||


 | Ideal sources for Wikipedia's health content are defined in the guideline Wikipedia:Identifying reliable sources (medicine) and are typically review articles. Here are links to possibly useful sources of information about Tianeptine.
|
| Text and/or other creative content from [[]] was copied or moved into [[]]. The former page's [ history] now serves to provide attribution for that content in the latter page, and it must not be deleted as long as the latter page exists. |
| The contents of the Selective serotonin reuptake enhancer page were merged into Tianeptine on 2014-04-25. For the contribution history and old versions of the redirected page, please see its history; for the discussion at that location, see its talk page. |
Opioid Affinity
editThe Ki values given are higher than codeine i.e. VERY WEAK. IF it has a strong opioid affect, it's a metabolite. I have seen an opioid with 2 aromatics with a dimethylamine on the bridging carbon. I seem to remember one of the organics being a pyridine and I THINK it had a m-OH on the benzene. Doxpicomine & Ciramadol both have 1 methylene between aromatics. There is analogue of ciramadol with a p-Cl in place of the m-OH. The Os of the -SO2-, like the N may have lone-pair interaction. Well, I will leave it with Chemoffice installed to overlay them. I would also be interested in the O to N to aromatic (so 2 choices - the further away one) and see how it matches nortilidine. The 7-membered ring will place the N further. — Preceding unsigned comment added by 213.106.56.145 (talk) 14:08, 14 December 2015 (UTC)
Placebo
edittianeptine has never undergone the gold standard i.e. testing against a tricyclic antidepressant compared against placebo. Why not,I do not know. I cannot believe that it has not been done as the first publication about tianeptine date from 1989 This site seems very close to the talk of pharmaceutic representative of Ardix. One should ask why this fantastic substance has not been approved by the FDA.
- Um, because the patent that Servier has on tianeptine has expired? Fortunately, Vela Pharmaceuticals (acquired recently by Pharmos) is interested. Yes, I know it's an...interesting website, but they're the only ones who've explained why Sevier hasn't tried marketing it in the US, besides the fact that so many people here have grown up on the idea that depression is merely a serotonin defiency. This is probably why Pharmos is marketing it for irritable bowel syndrome.--Rmky87 21:08, 8 July 2006 (UTC)
A strong antidepressant?
editUnlike neuroleptics or anxiolytics/(minor) tranquilizers, antidepressants effectivity can't be quantified by any way. An antidepressant either works in a depressive patient, or it does partially or not at all. There were and are some approaches to qualify particular drug for particular conditions of depressive disorder (e.g. classical tricyclics, such as imipramine, amitriptyline or clomipramine for severe major depression, or maprotiline for somatised ("larved depression" by Kielholz) depression, or SSRI's for anxiety- and/or OCD-accompagnied depression or high-dosed venlafaxine for torpid adynamic depressive disorders etc.), but in fact, none of these are much reliable. If you say "strong neuroleptic/antipsychotic", I would most likely imagine either a neuroleptic of high neuroleptic potency/with high chlorpromazine index, such as haloperidol, benperidol or fluphenazine, or a neuroleptic/antipsychotic, that works in psychotic patient that is refractory to many other drugs (such as clozapine). If I read "strong tranquilizer", I associate a potent benzodiazepine, like lorazepam, clonazepam or alprazolam.
But what is a "strong antidepressant"? The one that needs low relative doses (in mg/day)? Than, probably reboxetine and (S)-citalopram would be the most potent (doses of 4-12 mg/day and 5-20mg/day, respectivelly). Or the one that works for patients that are refractory to others and there is a statistically relative occurence of such algorithm, as in case of clozapine in antipsychotic-refractory schizophrenic psychoses? None of these criteria fits for tianeptine, and they are not relevant. Tianeptine is, according to the prescribing information of the manufacturer, suitable for treatment of medium-severe depressions without psychotic features, in somatic and anxiety comorbidities, and in the treatment of alcoholics or illcit drug dependant patients. I don't see any reason to mark the antidepressant effects of tianeptine as "strong", or, vice versa, why not to mark antidepressive effects of e.g. amitriptyline, clomipramine, dibenzepine, sertraline, mirtazapine or venlafaxine as "strong".
As I wrote, the only thing that makes an antidepressant "strong/potent" is the extent, in which it alleviates the symptoms of depressive disorder in every single patient, and thus is necessarily highly individual.--Spiperon 21:36, 15 October 2006 (UTC)
- I partially agree. The use of the term "strong" is not supported, as it is too vague. In my experience, people colloquially take this to mean "unselective" or "lots of side-effects".
- However, there are objective metrics to the efficacy of an antidepressant medication. For instance, tranylcypromine achieves remission in 85% of treatment refractory (i.e. failed to respond to 3 prior drugs in trials of adequate dose and duration), and is comparable to ECT. Imipramine is also quite effective, although the side-effects are often intolerable. If you could deliver 60mg cocaine over a 24 hour period with a slow-release capsule or a patch, along with something to counter its toxicity, you'd probably see even better stats, although that strays into the territory of definite abuse potential.
- The question is really how likely the drug is to be effective in a randomly selected patient in clinical practice, given adequate doses over an adequate period of time, as well as how long this improvement is likely to last.
- However, that question is only rarely answered, as drug trials have strict inclusion and exclusion criterion (more than one specialist has commented that you never encounter these patients in a clinical setting), and usually have a limited duration (typically 6 months or less). Basically, the question is actively sidestepped by the manufacturers. This makes financial sense, much in the same way as not actively comparing with antidepressants that are viable and on-patent. TCAs are preferred, with at least one source citing imipramine as the "gold standard". Many still use only inactive placebo or only TCAs, making the dataset harder to verify for inclusion in a meta-analysis.
- The availability of secondary sources on this aspect is thus generally limited to older drugs, such as the unselective MAOIs and the TCAs, most of which have been thoroughly studied.
- Therapeutic interval is not a good metric, as you pointed out, both due to the difference in Ki values (e.g. NE Ki >10000nM/L for reboxetine vs apx 4000nM/L for methamphetamine), absorption, half-life, etc. and such things as the balance between increased tonus and increased phasic transmission.
- In short, the word "strong" should not be used to describe any antidepressant. "Potent" could possibly be used in the sense that it is used with other drugs (degree of activity at the given receptors). All in all, however, there is a good argument that tianeptine can be a more effective drug than many others on the market, based on good efficacy at the recommended dose and an apparently large therapeutic index.
- Zuiram 05:20, 25 February 2007 (UTC)
How does it work?
editCan someone address the obvious contradiction? 68.0.113.54 05:17, 30 January 2007 (UTC)
- And what would that be?--Rmky87 21:33, 30 January 2007 (UTC)
- (S)he is probably referring to the serotonin hypothesis, and the apparent contradiction between the SSRIs showing antidepressant efficacy and tianeptine showing the same, despite the opposite mode of action.
- The party line is that the increased reuptake of 5HT from the synapse causes a buildup of 5HT in the vesicles. This would be a somewhat plausible explanation if the effect were similar to the SSRIs, as a significant amount of 5HT is destroyed by MAO-A in the synapse under usual circumstances. With faster reuptake, you would see less 5HT destroyed, and consequently a similar increase in stored 5HT as is seen with MAO-inhibitors.
- This theory is not as simple as it seems, however. SSRIs appear to owe their antidepressant efficacy to an upregulation of the postsynaptic D2-receptors in downstream systems, along with a downregulation of central beta-receptors. The former has a mood-brightening effect, while the latter has the effect of lessening the impact of emotional context in stored memories. Also, there may be some lessening of emotional lability due to downregulation of non-D2 dopamine-receptors; this would explain the potential for akathisia, through the same mechanism as the neuroleptics (reducted transmission at D4 receptors, if memory serves).
- Tianeptine would presumably give a moderate, but fairly rapid, increase in tonic and phasic dopaminergic activity (accounting for the high-dose abuse potential) due to disinhibition, followed by a longer term increase in vesicular storage of 5HT with a subsequent increase in phasic 5HT activity without the tonic increase seen with SSRIs and MAOIs. Again, it's been a while since I researched tianeptine, so my memory may not be an accurate guide here.
- There is no contradiction, though.
- Zuiram 05:33, 25 February 2007 (UTC)
- Could you (or someone else) write a bit about this in the article? --137.205.76.219 16:53, 17 March 2007 (UTC)
- I agree that an expansion (if only theoretical) would be helpful as little other action information appears on web searches. Also given the drugs use in erectile dysfunction could comment be made on its action in this regard cf SSRIs?
- I went through Serotonin withdrawal (so called Serotonin syndrome) because of being withdrawn from Clomipramine too quickly. The effects were a bit extreme and not altogether unpleasant. I asked the doctor and did my own research and the explanation was a lowered number of receptors for serotonin in the brain from the bodies natural tendency to be adaptive to the bioavailable levels. I started wishing for a drug with a short duration that reduced available serotonin in order to instigate small periods of Serotonin syndrome and thus eventually force the brain to increase the number of receptors beyond it's trained baseline. Tianeptine is short lived and lowers serotonin levels. Could it be forcing the receptor levels up?
- The euphoria described by patients is easy to believe; my experiences with serotonin withdrawal left me energized and extremely horny. I saw somewhere that being in love men's brain chemistry increases to induce cuddling (oxytosin/serotonin increases - I can't remember) and in women there was serotonin decreases to encourage them to higher sex drives. Just some thoughts and WK:OR so these thoughts would need to be sourced. (done anonymously on purpose) 71.86.156.73 (talk) 12:45, 9 August 2009 (UTC)
- I feel the need to mention (even though this comment was written a long time ago) that Serotonin Syndrome is NOT the same as SSRI Discontinuation Syndrome (ie., antidepressant withdrawal). Serotonin Syndrome is a potentially life-threatening condition, Discontinuation Syndrome just sucks. ;) Kailey elise (talk) 13:56, 18 December 2011 (UTC)
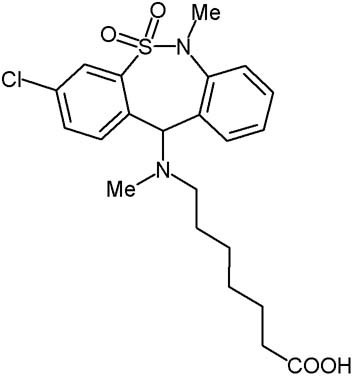
The molecular image is still wrong.
editIs someone going to fix this at some point? The conspicuous lack of chlorine anywhere in the image should have clued in anyone who actually looks at it.
When someone finally does attempt to fix it, please note:
http://www.biopsychiatry.com/tianeptine/tianeptine.jpg
{kind=link}
This image is also wrong. Count the carbons.
http://www.genome.jp/dbget-bin/www_bget?dr+D02575
This image is correct.
--76.209.58.121 14:34, 27 February 2007 (UTC)
- Fixed, thank you for noticing. Fvasconcellos 16:56, 27 February 2007 (UTC)
The image of the molecule lack methyl group bounded to nitrogen — Preceding unsigned comment added by 2A02:A316:6146:6E00:307D:A61E:379B:F2E (talk) 07:53, 23 February 2022 (UTC)
Irritable Bowel Syndrome/US Approval Process
editVera pharmaceuticals obtained a patent on the drug in the U.S. (for irritable bowel syndrome) and is going through the approval process to try to pass it through the FDA.
Tianeptine is not approved in the United States for any indication and has significant risks associated with it. https://www.fda.gov/consumers/consumer-updates/tianeptine-products-linked-serious-harm-overdoses-death
History of Tianeptine: Rejection in America
editAnyone skilled/knowledgeable enough to search and document how and why Tianeptine hasn't been submited/approved in USA/Canada ? Marty (whereismarty@hotmail.com) 69.70.202.20 (talk) 20:39, 2 June 2008 (UTC)
- "It is not marketed in North America because its patent has expired. To gain a US product license, a raft of costly new clinical trials would be needed by the FDA. Unfortunately, American regulators are habitually sceptical of the calibre of European medical science." That source is of unknown quality. Since it is at tianeptine.com it could be profit motivated. 71.86.152.127 (talk) 17:46, 27 September 2009 (UTC)
- It has also been said (I don't remember the source) that American and European drug companies tend to "respect each other's turf", that is, they don't try to push medicines on each other continents, in part because both of them are assumed (correctly IMO) to be favored by the regulatory bodies in their respective regions, so that a European drug will have a harder time getting approved when there is an American drug for the same condition and vice versa (so that often it doesn't make economic sense even to try to get things approved on the other side of the Atlantic). Historian932 (talk) 03:26, 21 June 2011 (UTC)
Abuse
editMoved the part about abuse in Russia into the abuse section. Also, there's no hits for "tianeptine abuse" (or even "tianeptine") on Google News, so I added a citation needed tag. Apophenic (talk) 20:43, 30 October 2008 (UTC)
- There's a video going around showing the potential side effects of intravenous tianeptine injection.
- No way to know what that is without speaking Russian, of course. One of the subjects makes a motion as if to say he injected the tianeptine into his hand, between the fingers. The effects of whatever they injected are quite shocking. Skin dissolved right to the bone...
- 24.68.36.117 (talk) 07:28, 31 May 2009 (UTC)
- there's zero evidence even to support that this has anything to do with tianeptine. for all we know they injected motor oil into their veins. it's important to note that the video mentioned is very graphic, quite disgusting, and not for the faint of heart. for that matter, i've removed the link to the video, since it has no demonstrated connection to this article. there's no point in spreading misinformation, based on a shock-website that claims something. if a russian speaker provides an actual translation, fine, then maybe it's worth further review. until then, just as the site name suggests, it's 'totally crap'. Anastrophe (talk) 18:02, 31 May 2009 (UTC)
- And, of course, it somehow (in some f****d up fantasy world of yours) matters what website it is hosted on when it's obvious that physicians are treating the patients in the video. If what the doctors are saying backs up claims that Tianeptine was the culprit, why should it be dismissed? Just because you don't feel like asking for someone to translate it doesn't mean you should be an a*****e and claim it's bogus. Do you speak Russian? Are you a physician? Then how the hell would you know? It's self-righteous a******s like you that are ruining wikipedia. 66.153.217.152 (talk) 08:11, 11 June 2009 (UTC)
- O yeah... that tirade helped prove your point. 71.86.152.127 (talk) 17:38, 27 September 2009 (UTC)
- And, of course, it somehow (in some f****d up fantasy world of yours) matters what website it is hosted on when it's obvious that physicians are treating the patients in the video. If what the doctors are saying backs up claims that Tianeptine was the culprit, why should it be dismissed? Just because you don't feel like asking for someone to translate it doesn't mean you should be an a*****e and claim it's bogus. Do you speak Russian? Are you a physician? Then how the hell would you know? It's self-righteous a******s like you that are ruining wikipedia. 66.153.217.152 (talk) 08:11, 11 June 2009 (UTC)
- there's zero evidence even to support that this has anything to do with tianeptine. for all we know they injected motor oil into their veins. it's important to note that the video mentioned is very graphic, quite disgusting, and not for the faint of heart. for that matter, i've removed the link to the video, since it has no demonstrated connection to this article. there's no point in spreading misinformation, based on a shock-website that claims something. if a russian speaker provides an actual translation, fine, then maybe it's worth further review. until then, just as the site name suggests, it's 'totally crap'. Anastrophe (talk) 18:02, 31 May 2009 (UTC)
I am Russian. Tianeptine is a Schedule III drug in Russia since 2010. Illigal possesion of it is a criminal offence. Regarding the videos circulating on the net showing necrosis following injections of tianeptin, this is because the victims injected themselves with water suspention of crushed tablets and did this often into arteries instead of veins. Non-soluble components cementing a tablet blocked the blood flow in capillaries resulting in necrosis. — Preceding unsigned comment added by 92.246.185.158 (talk) 17:21, 12 October 2011 (UTC)
- These effects are however not caused by tianeptine. If those addicts would inject crushed up Vitamin B1 tablets that way, the results would most likely have been comparable.--78.43.34.138 (talk) 22:32, 11 November 2011 (UTC)
- While this is true, no one's injecting Vitamin B into their veins in hopes of relieving their opioid withdrawals, like they do with Coaxil in Russia. However, I've been informed by others who are privy to what the junkies in Russia are actually up to these days, that much of this flesh-eating disgustingness is due to "krokodil" or something similar, which is NOT the injection of Coaxil, but is the injection of a grossly unclean attempt at making desomorphine via codeine tablets. While it seems to use something very similar to the RP/I method of making methamphetamine, it is NOT cleaned up in any way. So people are injecting lots of caustic chemicals along with their alleged desomorphine. *shudder* Perhaps the people desperate enough to inject this concoction are also more likely to inject Coaxil, and thus the rumor that Coaxil is solely to blame for this condition was born? Kailey elise (talk) 14:03, 18 December 2011 (UTC)
- These effects are however not caused by tianeptine. If those addicts would inject crushed up Vitamin B1 tablets that way, the results would most likely have been comparable.--78.43.34.138 (talk) 22:32, 11 November 2011 (UTC)
3D formula
editThe 3D formula ist wrong since only one of the two enantiomers is shown. Tianeptine is a racemate. Best regards, --Jü (talk) 17:45, 25 July 2012 (UTC)
Merging article SSRE into Tianeptine
editHello everybody,
I placed a merge from tag in the Tianeptine article, because the article selective serotonin reuptake enhancer (SSRE) is about nothing else than tianeptine, and in addition, it's whole justification comes from an outdated theory (that tianeptine's antidepressant effect comes from enhanced serotonin reuptake). I suggest to copy what's worth to include in the tianeptine article, and afterwards replace the content of SSRE by a forward to tianeptine. The redundancy of both articles is a maintenance obstacle.
Best, --Richard (talk) 18:14, 2 March 2014 (UTC)
- I wouldn't call the theory outdated, per se, I realise there are other actions that have recently come to light but still it hasn't been proven that this isn't a contributing factor; but I do agree with you I think the two should be merged. Plus tianeptine isn't truly a selective serotonin reuptake enhancer, it also enhances norepinephrine's reuptake. (PMID: 15361747) Fuse809 (talk) 11:44, 6 March 2014 (UTC)
- Do you have access to the full article with PMID 15361747? If so, please share which are the 4th and 5th cite in this article, because I found no source for a norepinephrine reuptake enhancing mechanism of Tianeptine. The term monoamine reuptake enhancer can't be justified just by the title of a paper. Sheldon Preskorn is a MD, who doesn't do this research on his own. Best --Richard (talk) 10:13, 11 March 2014 (UTC)
- Thx, but when they don't mention effects on norepinephrine reuptake, then the 1st sentence in Tianeptine#Mechanism of action should be edited again. --Richard (talk) 21:12, 11 March 2014 (UTC)
- I'd suggest keeping the pages apart and simply note that the theory is outdated on the SSRE page. This page should evolve without the baggage of the, now empty, SSRE class of drugs. Seppi333 (Insert 2¢ | Maintained) 16:09, 6 March 2014 (UTC)
- It's not meaningful to keep an article stub which only mentions that some medication was once thougt to be the only class member. A new SSRE article could easily be written, if an SSRE would be developed. One could redirect SSRE to a stub serotonine reuptake enhancer (SRE), whith Tianeptine as the only class member (and without the redundancy to Tianeptine). But even if Tianeptine has SRE property isn't sure (PMC 2902200), as it is not known/scientifically debated if Tianeptine really enhances serotonin reuptake or even decreases the serotonin-level for longer as the beginning of a treatment (an effect that occours also frequently in SSRI). So I'm still thinking it's best to forward to Tianeptine, where already is written, that it was called a Serotonin Reuptake Enhancer. Best --Richard (talk) 10:13, 11 March 2014 (UTC)
I would like to close discussion and start merging. There is still an article reuptake enhancer (RE), which isn't redundant to tianeptine, and which mentions it. This article lists one other drug that seems to posses a reuptake mechanism (not for serotonin), scratch along to be an article. That's at least better as an own class for just one drug. I hope it evolves over time to more than a stub, when coluracetam and tianeptine getting better understood, or more RE will be dicovered. But most of the SSRE article is redundant to tianeptine, and the rest is contained in RE or should be transfered to this article. Best --Richard (talk) 15:23, 9 April 2014 (UTC)
CVS effects
editWe have a seemingly contradictory statements in the article: on the one hand, the lead paragraph mentions "a relative lack of sedative, anticholinergic and cardiovascular adverse effects"; the reference in the section 'Side effects' states that the proarrhythmogenic effects of tianeptine have not been well studied. Should we rectify the lead? --Eleassar my talk 10:13, 13 February 2016 (UTC)
Tianeptine in combination w/ MAOIs
editI added a caveat that tianeptine is more than safe to use concurrently with MAOIs because there is no pharmacological contraindication. Tianeptine lacks any serotonergic/noradrenergic activity that would make this combination unsafe. If you would like to challenge me, please go ahead because there are no actual reports of an unsafe interaction transpiring with MAOIs; there is so much misinformation regarding MAOIs permeating psychiatry it's mind boggling, it's no better than sheer hysteria.
47.184.211.178 (talk) 20:24, 11 March 2019 (UTC)Tim s.
Use of incorrect pharmacodynamic terms
editIn the section listing tianeptine's affinity at various targets, the table is labelled Ki. Ki refers to inhibition and is clearly not applicable when describing an agonist (such as at MOR Kd should be used). Unfortunately this error seems to be prevalent across wikipedia.
Wdhiwhfwaih (talk) 01:47, 14 March 2021 (UTC)
Incorrect chemical structure
editsolved already.
Structural analog of Schedule I Amineptine
editAlthough it was removed because someone disagrees because nobody has been arrested for it yet, I will just post it here.
Tianeptine is a structural analog of Amineptine which is a Schedule I. It does not matter that Amineptine was scheduled 2 years ago. It does not matter that the DEA hasn't arrested anyone for Tianeptine under the federal analog act yet. Per the way the federal analogue act is defined in the USA it only needs to meet a structural basis. It does not have to be functionally similar. It's as simple as "yes, that's a structural analog of this substance." They're structural analogs of eachother and that's all they need and that's why it should be noted on the article so people can take the right steps to protect themselves. — Preceding unsigned comment added by Gettinglit (talk • contribs) 21:36, 27 May 2023 (UTC)
- The analogue act varies greatly on a case-by-case basis, but if we are to cast our judgement on whether it could meet the criteria of the law regarding the structure alone, this is what the actual text is:
(i) the chemical structure of which is substantially similar to the chemical structure of a controlled substance in schedule I or II
- Not if it is an analogue or not in reality. I think tianeptine would meet this criteria in relation to amineptine, but a better solution would be to write something like "could be considered schedule 2 as an analogue of amineptine under the Controlled Substance Analogue Enforcement Act" to acknowledge that this criteria is usually determined by factors other than the structure itself and the degree of subjectivity in actual cases. Towelbin (talk) 03:30, 28 May 2023 (UTC)