| Lower Bones | |
|---|---|
 Lateral aspect of right leg | |
| Details | |
| Identifiers | |
| Latin | membrum inferius |
| Anatomical terminology | |
Article title - Lower Bones
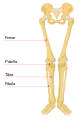
Lower bones refer to the bones on the lower limb. It consists of three groups including the thigh, the leg and the foot. The group of the thigh is positioned from the hip and the knee; the group of the leg which is placed between the knee and the ankle; and the group of the foot on the bottom side of the ankle joint. The femur bone is the single long bone within the lower limb. The tibia (medially) and the fibula (laterally) are the paired bones of the lower leg. The patella is considered as the kneecap in the human body, articulated with the femur bone and located on the front of the knee joint. The foot bones are made up of tarsals (7), metatarsals (5) and phalanges (14)[1].
Femur
editStructure
editThe femur is the single long bone in the upper leg, also named thigh bone anatomically. It is the longest and heaviest bone in the human body. The length of the femur plays an important role in body height, approximate 26.75% on average. [2]. It is located between the hip bone and knee. Proximally, the femur is characterised by the smooth and round-shaped head, which connects with the acetabulum of hip bone forming the ball and socket joint. [3]. The neck of the femur is about 135 degrees which articulate with the head and the shaft and contributes to the walking. [4]. The areas of bony projection are called greater and lesser trochanters, which are the site of various muscle attachment.[3]. Distally, the shaft extends to form two condyles, which articulates with the proximal tibia to form the knee joint[4]. The patella is a sesamoid bone, which is formed by extending two condyles.[1].
Function
editIn terms of the function, the femur bone is mainly responsible for bear-weight and provide stability to the human body. The head of the femur is used to bear body weight of upper bones. The structure of capsular ligament plays an important role in the human body such as external rotation [5]. In relate to the knee joint, cruciate ligament allows for rotation[5]. The patellofemoral joint is applied to extend the knee [5].
Clinical Significance of the femur
editThe deformed long bone is resulting from the disease: rickets[5]. During rickets, endochondral ossification will be reduced, and bone growth will become slow. Rickets is caused by various reasons such as lack of vitamin D, low Ca2+ intake and sun exposure decrease[5].
Tibia
editStructure
editThe lower region consists of tibia and fibula bones. The tibia also called the shin bone and is the only bone that connects to the distal femur[3]. It is the second bone in the lower limb because of its weight-bearing[1]. Its length is about 21.3% on average of the body heightCite error: The <ref> tag name cannot be a simple integer (see the help page).. In the proximal, there are medial and lateral condyles that are part of the knee joint. The intercondylar eminence that is an irregular shaped structure and used to support the ligament of the knee joint [6]. Compared with the lateral condyle, the medial condyle is larger and is used to support the tibial shaft that is triangular-shaped in cross-section Cite error: The <ref> tag name cannot be a simple integer (see the help page).. In the shaft of the tibia, found three borders (anterior, interosseous and lateral) and three surfaces (anterior, medial and lateral) [7]. The patella ligament is formed to the tibial tubercle and contributes to the knee joint. In the distal, there is a large bony prominence called the medial malleolus (medially), found on the ankle joint[6]. There is also a groove area known as fibula notch (laterally) on the distal of the tibia[6].
Function
editTibia bone is the second-long bone in the human body[1]. The primary function is bearing the body weight of the human[1]. In terms of the movement of the tibia, flexion and extension can be created as well as plantarflexion and dorsiflexion can be allowed.
Development
editThe tibia bone contains the structure called ossification centres which is developed in the seventh week[8]. One of the ossification centres is used for the diaphysis and other two is used for epiphysis[8]. The development of the ossification centres is slightly different between male and female. For male, it closes at age 18 while ossification centres for female close at age 16[8].
Blood supply
editThe blood supply to the tibia bone contain two vessels which are named nutrient artery and periosteal vessels[8]. The origin of the nutrient artery is located in the dorsal side of the tibial artery, it flows into the distal bone and enter the soleal line[8]. The origin of the periosteal vessels is placed in the ventral side of the tibial artery[8].
Fibula
editStructure
editThe fibula is placed on the lateral side of the tibia bone. The fibula and the tibia are connected by an interosseous membrane[7]. Compared to the tibia, the fibula is much slender and smaller as well as it does not contribute to the knee joint[7]. The most important thing is that it does not link with the femur bone, but it does form the part of the ankle joint and support the muscles of the lower leg[6]. The fibula consists of the head, the neck, the shaft and the distal end. Proximally, the head of the fibula is large and round-shaped and articulated with the lateral side of the tibia to create the proximal tibiofibular joint[6]. Due to muscle attachments, the shape of the shaft is constantly changing form triangular-shaped to irregular-shaped. The intermediate tibiofibular joint is formed and located between the shaft of the tibia and the fibula[1]. Distally, it is noted that has a prominent surface called lateral malleolus, which connects to the talus of the foot bone[6]. This lateral projection forms a part of the ankle. The distal tibiofibular joint is formed between the tibia and the fibula at the fibula notch[6].
Function
editThe main function of the fibula bone is that combine with the tibia bone and used to stabilize the ankle joint[9]. It also creates leverage via several grooves during the movement of the ankle joint[9]. Other structure such as collateral ligament in the lateral side provide stability for the knee joint[9].
Clinical significance of the fibula
editThe clinical significance of the fibula is reflected in congenital and neurological. From the congenital perspective, the bone age of infants can be estimated by measuring the length of the fibular shaft. [10]. The deficiency of fibula is resulting from the fibular hypoplasia-aplasia. [11]. It can be diagnosed at birth if there is a dramatical difference limbs length. Additionally, fibular nerve (also called the common peroneal nerve) is located the lateral and posterior to the neck of the fibula. Destroyed fibular nerve would cause entrapment neuropathy. [12]. The main symptoms contain foot drop and loss of sensory on the legs.
Foot bones
editStructure
edit
The feet are a much more mobile and flexible structure. It consists of 26 bones which are divided into three sections: the hindfoot, midfoot and forefoot. [13]. The hindfoot contains talus and calcaneus. The talus is the single bone that articulates with the fibula and the tibia. The weight of the human body can be transmitted from talus to the calcaneus. The calcaneus is the largest bone within the tarsal groups. The midfoot consists of navicular, cuneiforms (3) and cuboid bone. [14]. The forefoot is made up of five metatarsals and phalanges (proximal, middle, distal[13]. The metatarsals are numbered 1-5 (I-V) from medial to the lateral side and each metatarsal bone contains a head, shaft and a base[13]. The metatarsals (1-3) articulate with the cuneiform bones[10]. The first metatarsal is particularly robust, as toe 1 is a weight-bearing structure. In the phalange bones, it is noted that toe 1 only has two phalanges (proximal, distal) while tow 2-5 have three phalanges[13].
Joint
editThere are four joints of the foot bones[6]. In functional classification, all joints in the foot are synovial joint.
Intertarsal joints are located between the tarsals. The articulated joint between three groups of bones (metatarsals, three cuneiforms, cuboid bone) is called tarsometatarsal joint, which allows inversion and eversion[6]. In mechanical classification, those two joints are plant or sliding joint[6]. The head of the metatarsals connects to the proximal phalanges to form the metatarsophalangeal joint, which is a condyloid or hinge joint[6]. The joint between phalange bones is known as an interphalangeal joint which is a hinge joint and allows flexion and extension[6].
Function
editThe foot plays an important role in the human body because of the weight-bearing structure. It not only provides the attachment of various muscle but also help to absorb force.
Artery supply of lower bones
editThe communication between a number of arteries is significantly important to maintain the blood supply in the human body. In the lower limb, the artery starts from the external iliac artery which is a branch of the common iliac artery. [15]. The external iliac artery supplies the superficial femoral artery and then supplies the deep femoral artery which supplies the blood to the muscles of the upper leg[15]. The deep femoral artery flows into the geniculate artery that can provide many branches to support the popliteal artery[15]. In the end, the popliteal artery flows into the artery of the tibia bone[15].
Development of the lower bones
editThe development of the lower bones is significantly complex. The human body is made up of upper limb and lower limb. The lower limb is communicated with upper limb via pelvic girdle which consists of two hip bones and sacrum. [16]. The bony pelvis is a robust ring structure, which is formed by connecting the pelvic girdle and the sacrum bone.
Function
editThere are two main functions of the lower bones. Firstly, the formation of the lower bones is effectively supporting the body weight. The muscles of the pelvic girdle and sacrum bone are importantly significant to support the body weight during standing or walking. The second function of the lower bones is locomotion which means the ability of movement from one place to another place. All of the bones, joints and muscles need to be cooperated to move the body. In the human body, sacroiliac joint plays an important role, as it is used to transfer the body weight to the pelvic girdle and the femur bone[16]. The femur bone is inclined in direction due to female have wider pelvis.
Development
editThe development of the lower bones needs to experience several stages. Initially, the embryo starts to develop and grow in the lower limbs. It is estimated that immature embryo is about 5 millimetres long[16]. In the fourth week, the immature embryo is formed after ovulation[16]. The development of the buds in the lower limb is slower than those of the upper limb. In the sixth week, the buds experience a change from ossification centres to the tibia bone and the fibula bone is formed during the seventh and eighth week[16]. The nerves begin to develop in the lower limb as well as the muscles and the bones start to differentiate. Eventually, the foot bone is formed, and the lower limb is compliantly developed.
Additional images
edit-
 Lower portion of a human skeleton
Lower portion of a human skeleton -
 View from the front.
View from the front. -
 Bones of the right leg. Anterior surface
Bones of the right leg. Anterior surface -
 Position of fibula (shown in red)
Position of fibula (shown in red)



References
edit- ^ a b c d e f Kapit, Wynn; Elson, Lawrence M. (1977). The anatomy coloring book. New York: Harper&Row. ISBN 978-0321832016.
- ^ Iscan, Mehmet Yasar; Steyn, Maryna (2013). The human skeleton in forensic medicine. United States: Charles C Thomas Publisher. p. 493. ISBN 978-0-398-08879-8.
- ^ a b c Gray, Henry (1878). Anatomy of the human body. Lea & Febiger.
- ^ a b Hoaglund, F. T.; Low, W.D. (1980). "Anatomy of the femoral neck and head, with comparative data from Caucasians and Hong Kong Chinese". Clinical orthopaedics and related research (152): 10-16.
- ^ a b c d e Chang, Amy; Hubbard, John B. (2018). "Anatomy, Bony Pelvis and Lower Limb, Femur". National Center for Biotechnology Information, U.S. National Library of Medicine. PMID 30422577.
- ^ a b c d e f g h i j k l Tortora, Gerard J.; Derrickson, Bryan (2017). Principles of anatomy & physiology. John Wiley & Sons. p. 250-253. ISBN 978-1-119-32064-7.
- ^ a b c Drake, Richard; Vogl, A. Wayne (2009). Gray's Anatomy for Students-Rental: With STUDENT CONSULT Online Access. Elsevier Health Sciences. ISBN 978-0443069529.
- ^ a b c d e f Bourne, Matthew; Murphy, Patrick B. (2018). "Anatomy, Bony Pelvis and Lower Limb, Tibia". National Center for Biotechnology Information.
- ^ a b c Gupton, Marco; Kang, Michael (2018). "Anatomy, Bony Pelvis and Lower Limb, Fibula". National Center for Biotechnology Information, U.S. National Library of Medicine. PMID 29261984.
- ^ a b Rastogi, R (2008). "Congenital Unilateral Bowing of Tibia and Fibula". Medical journal, Armed Forces India. 3 (64): 295–296. doi:10.1016/S0377-1237(08)80128-1. PMID 27408175.
- ^ Bedoya, Maria A.; Chauvin, Nancy A.; Jaramillo, Diego; Davidson, Richard; Horn, B. David; Ho-Fung, Victor (2015). "Common Patterns of Congenital Lower Extremity Shortening: Diagnosis, Classification, and Follow-up". Radiographics. 4 (35): 1191-1207. doi:10.1148/rg.2015140196.
- ^ Marciniak, Christina (2013). "Fibular (peroneal) neuropathy: electrodiagnostic features and clinical correlates". Physical Medicine and Rehabilitation Clinics. 1 (24): 121-137. doi:10.1016/j.pmr.2012.08.016. PMID 23177035.
- ^ a b c d Aiello, Leslie; Dean, Christopher (1990). An introduction to human evolutionary anatomy. Academic Press. p. 395-428. ISBN 9780120455911.
- ^ Saladin, Kenneth S. (2005). Human anatomy. Rex Bookstore: McGraw-Hill. p. 213-221. ISBN 978-007-125971-2.
- ^ a b c d Bhatt, Deepak L (2004). Guide to Peripheral and Cerebrovascular Intervention. London: Remedica: Remedica Publishing. ISBN 1-901346-61-7.
- ^ a b c d e Jacob, Sam (2007). Human anatomy: a clinically-orientated approach. Elsevier Health Sciences. p. 135-179. ISBN 9780443103735.