Angiofibroma (AGF) is a descriptive term for a wide range of benign skin or mucous membrane (i.e. the outer membrane lining body cavities such as the mouth and nose) lesions in which individuals have:
- benign papules, i.e. pinhead-sized elevations that lack visible evidence of containing fluid;
- nodules, i.e. small firm lumps usually > 1 mm in diameter; and/or
- tumors, i.e. masses often regarded as ~8 mm or larger.
| Angiofibroma | |
|---|---|
 | |
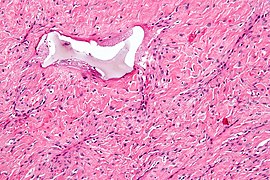
| Angiofibroma, Hematoxylin and eosin stain, magnification ×10. | |
| Specialty | Oncology |
| Symptoms | Itchiness and sometimes bleeding.[1] |
| Complications | Facial disfigurement and stigmatization.[1] |
| Causes | Local overgrowth of collagen, fibroblasts, and blood vessels.[1] |
| Risk factors | Tuberous sclerosis, Birt-Hogg-Dubé syndrome, and Multiple endocrine neoplasia type 1.[1] |
| Diagnostic method | Skin biopsy.[1] |
| Differential diagnosis | Intradermal melanocytic naevus, Acne, Basal cell carcinoma, Viral warts, Subungual exostosis, Molluscum contagiosum, and Anogenital warts.[1] |
| Treatment | Excision, Dermabrasion, Using lasers, electrical, and radiofrequency devices, Cryotherapy, Topical podophyllotoxin, Topical rapamycin, and Topical beta-blockers.[1] |
Diagnosis
editAGF lesions share common macroscopic (i.e. gross) and microscopic appearances. Grossly, AGF lesions consist of multiple papules, one or more skin-colored to erythematous, dome-shaped nodules, or usually just a single tumor. Microscopically, they consist of spindle-shaped and stellate-shaped cells centered around dilated and thin-walled blood vessels in a background of coarse bundles of collagen (i.e. the main fibrous component of connective tissue).[2] Angiofibromas have been divided into different types but commonly a specific type was given multiple and very different names in different studies.[2]
Cutaneous angiofibroma
editThese papule, nodule, and/or tumor lesions occur on the: 1) face and are typically termed fibrous papules; 2) penis and are typically termed pearly penile papules; and 3) underneath a fingernail or toenail and are typically termed periungual angiofibromas. Some of these cutaneous AGF lesions occur in individuals with one or more of 3 different genetic diseases: tuberous sclerosis, multiple endocrine neoplasia type 1, and Birt-Hogg-Dube syndrome.[3] The following are examples of these cutaneous angiofibromas and their alternate names.
Fibrous papules
editFibrous papules are also termed facial angiofibromas and were formerly and incorrectly termed adenoma sebaceum (fibrous papules are unrelated to sebaceous glands[4]). They develop in up to 8% of the general adult population and occur as 1 to 3[5] pink to red,[4] dome-shaped papules in the central areas of the face, nose, and/or lips.[6] About 75% of individuals with tuberous sclerosis present with fibrous papules in their infancy or early childhood; when associated with this rare disease, the lesions often occur as multiple papules[5] in symmetrical, butterfly-shaped patterns over both cheeks and the nose.[7] Fibrous papules also occur in individuals with multiple endocrine neoplasia type 1 (a study done in Japan found that 43% of individuals with this genetic disease bore facial angiofibromas)[8] and, uncommonly, in individuals with Birt-Hogg-Dube syndrome.[9]
Pearly penile papules
editPearly penile papules are also termed papillae coronae glandis and hirsutoid papillomas. The condition of having such papules or papillae is called hirsuties papillaris coronae glandis or papillomatosis coronae glandis or papillomatosis coronae penis.[10] These lesions develop in up to 30% of males during their puberty or, less commonly, early adulthood. They typically occur as numerous white-colored to skin-colored papules located circumferentially around the corona of the penis or, less commonly, the ventromedial aspect of the corona near the penis's frenulum.[11] (Vestibular papillomatosis, also named hirsutoid vulvar papillomas, vulvar squamous papillomatosis, micropapillomatosis labialis, and squamous vestibular micropapilloma, is the female equivalent of pearly penile papules in men.[12] It has not been formally termed an angiofibroma.)
Periungual angiofibromas
editPeriungual angiofibromas are also termed Koenen's tumors, periungual fibromas, and subungual fibromas.[13] In addition, these tumors were formerly regarded as a type of acral angiofibroma (see below description).[14] These lesions present as multiple nodules or tumors under multiple finger and/or toe nails of individuals with tuberous sclerosis[4] or in one case the Birt-Hogg-Dube syndrome.[15] Periungual angiofibromas have also been reported to occur in individuals that do not have these genetic diseases.[16] Periungual angiofibromas tumors can be highly mutilating finger/toe-nail lesions.[4]
Oral fibromas
editOral fibromas are also termed irritation fibromas, focal fibrous hyperplasia, and traumatic fibromas.[17] These lesions are nodules that occur on the buccal mucosa (i.e. mucous membranes lining the cheeks and back of the lips) or lateral tongue.[18] They may be irritating or asymptomatic and are the most common tumor-like lesions in the oral cavity. Oral fibromas are not neoplasms; they are hyperplastic (i.e. overgrowth) reactions of fibrous tissue to local trauma or chronic irritation.[19]
Nasopharyngeal angiofibromas
editNasopharyngeal angiofibromas, also termed juvenile nasopharyngeal angiofibromas, fibromatous hamartomas, or angiofibromatous hamartoma of the nasal cavity, are large benign tumors (average size 5.9 cm in one study) that develop almost exclusively in males aged 9 to 36 years old. They commonly arise in the nasopharynx (i.e. upper part of the throat that lies behind the nose) and typically have attachments to the sphenopalatine foramen, clivus, and/or root of the pterygoid processes of the sphenoid bone. These tumors may expand into various other nearby structures including the cranial cavity.[20] Nasopharyngeal angiofibromas are highly vascularized tumors consisting of fibroblasts (i.e. connective tissue cells) in a dense collagen matrix (i.e. tissue background). Studies have suggested that these tumors are due to the expression of male sex hormones (i.e. androgens and progesterones), genetic factors, molecular alterations (i.e. changes in the normal characteristics of cells that lead to abnormal cell growth), and/or human papillomavirus infection.[21]
Angiofibroma of soft tissue
editAngiofibroma of soft tissue is also named angiofibroma, not otherwise specified, by the World Health Organization, 2020. The Organization also classified these lesions as in the category of benign fibroblastic and myofibroblastic tumors.[22] These tumors more often afflict females,[23] typically occur in adults (median age 49 years), have a median size of ~3.5 cm, and develop in a leg near to, and may invade, a large joint. Less uncommonly, they occur in the back, abdominal wall, pelvic cavity, or breast. Angiofibroma of soft tissue tumors consist of uniform, bland, spindle-shaped cells and a prominent vascular network consisting of small thin-walled branching blood vessels in a variably collagenous tissue background. Its tumor cells contain an AHRR-NCOA2 fusion gene in 60% to 80% of cases and a GTF2I-NCOA2 or GAB1-ABL1 fusion gene in rare cases.[24]
Cellular angiofibroma
editCellular angiofibroma is usually a small, slow-growing tumor arising in the vulva-vaginal areas of adult woman and the inguinal-scrotal areas of adult men although some of these tumors, especially in men, can grow up to 25 cm. Affected men are usually older (7th decade) than women (5th decade).[25] Less commonly. cellular angiofibromas have occurred in various other superficial soft tissue areas throughout the body.[26] These tumors are edematous (i.e. abnormally swollen with fluid), highly vascular, spindle-shaped cell lesions with a variable amount of fibrous stroma.[25] In 2020, the World Health Organization classified cellular angiofibroma tumors in the category of benign fibroblastic/myofibroblastic tumors.[22] The tumor cells in these lesions contain chromosome and gene abnormalities including a loss of one of the two RB1 genes. It has been suggested that the loss of this gene contributes to the development of cellular angiofibroma tumors.[27]
Acral angiofibromas
editAcral angiofibromas are also termed superficial acral fibromyxomas, digital fibromyxomas, acquired digital fibrokeratomas, acquired periungual fibrokeratomas, garlic clove fibromas,[28] digital fibromas, and cellular digital fibromas.[14] At one time, periungual angiofibromas were regarded as a type of acral angiofibroma (see above description).[14] Acral refers to distal sites of the ears, nose, hands, fingers, feet, and toes. Acral angifibromeae occur primarily in areas close to the nails of fingers and toes (~80% of cases)[28] or, less commonly, palms of the hands or soles of the feet.[14] The tissues of this tumor consists of bland spindle-shaped and star-shaped cells within a collagen fiber-rich stroma containing prominent blood vessels and mast cells.[28]
- Photos
-
 Glans penis with Hirsuties papillaris penis. Papules are common on uncircumcised penises.
Glans penis with Hirsuties papillaris penis. Papules are common on uncircumcised penises. -
 Koenen tumor in patient with tuberous sclerosis complex.
Koenen tumor in patient with tuberous sclerosis complex. -
 Photo of irritation fibroma on the labial mucosa.
Photo of irritation fibroma on the labial mucosa. -
 High magnification micrograph of a nasopharyngeal angiofibroma.
High magnification micrograph of a nasopharyngeal angiofibroma. -
 Adenoma sebaceum. Multiple wart-like, waxy lumps consisting of angiomatous and fibrous tissue associated with tuberous sclerosis.
Adenoma sebaceum. Multiple wart-like, waxy lumps consisting of angiomatous and fibrous tissue associated with tuberous sclerosis.





See also
editReferences
edit- ^ a b c d e f g "Angiofibroma: Types, Appearances and Causes — DermNet". dermnetnz.org. Retrieved 2023-10-28.
- ^ a b "Picture of Angiofibroma (Facial) on MedicineNet".
- ^ Macri, A.; Kwan, E.; Tanner, L. S. (2021). "Cutaneous Angiofibroma". StatPearls. StatPearls. PMID 29494077.
- ^ a b c d Zheng LQ, Huang Y, Han XC (May 2013). "Angiofibromas with multiple epidermoid cysts in tuberous sclerosis: new mutation or post-traumatic?". Journal of Cutaneous Pathology. 40 (5): 509–12. doi:10.1111/cup.12103. PMID 23418925. S2CID 28266318.
- ^ a b Klonowska K, Thiele EA, Grevelink JM, Thorner AR, Kwiatkowski DJ (October 2021). "Sporadic facial angiofibroma and sporadic angiomyolipoma mimicking tuberous sclerosis complex". Journal of Medical Genetics. 59 (9): 920–923. doi:10.1136/jmedgenet-2021-108160. PMID 34635572. S2CID 238635311.
- ^ Shi X, Zhang B, Ma L (July 2021). "Fibrous papules on the lips". Pediatric Dermatology. 38 (4): 954–955. doi:10.1111/pde.14610. ISSN 0736-8046. PMID 34184319. S2CID 235673971.
- ^ Krishnan P, Patel SM (2016). "Adenoma sebaceum: Dermatological finding unmasking central nervous system pathology". Journal of Pediatric Neurosciences. 11 (4): 378–379. doi:10.4103/1817-1745.199465. PMC 5314862. PMID 28217171.
- ^ Sakurai A, Matsumoto K, Ikeo Y, Nishio SI, Kakizawa T, Arakura F, Ishihara Y, Saida T, Hashizume K (October 2000). "Frequency of facial angiofibromas in Japanese patients with multiple endocrine neoplasia type 1". Endocrine Journal. 47 (5): 569–73. doi:10.1507/endocrj.47.569. PMID 11200937.
- ^ Sattler, E. C.; Steinlein, O. K.; Adam, M. P.; Ardinger, H. H.; Pagon, R. A.; Wallace, S. E.; Bean LJH; Mirzaa, G.; Amemiya, A. (1993). "Birt-Hogg-Dubé Syndrome". GeneReviews [Internet]. PMID 20301695.
- ^ Jha N (2021). "Coronavirus is Not the Only Corona We Know in Dermatology". Indian Dermatology Online Journal. 12 (1): 208–209. doi:10.4103/idoj.IDOJ_582_20. PMC 7982023. PMID 33768062.
- ^ Saardi KM, Dubin JM, Cardis MA (May 2021). "Images – Atypical presentation of pearly penile papules". Canadian Urological Association Journal. 15 (5): E301–E303. doi:10.5489/cuaj.6787. PMC 8095284. PMID 33119502.
- ^ Giuffrida G, Lacarrubba F, Boscaglia S, Nasca MR, Micali G (2019). "A Noninvasive Aid for Office-Based Gynecologists for the Diagnosis of Common External Genital Disorders". Obstetrics and Gynecology International. 2019: 1830245. doi:10.1155/2019/1830245. PMC 6816007. PMID 31737074.
- ^ Oba MÇ, Uzunçakmak TK, Sar M, Serdaroğlu S (March 2021). "Dermoscopic findings in a case of multiple subungual fibromas". Acta Dermatovenerologica Alpina, Pannonica, et Adriatica. 30 (1): 35–37. doi:10.15570/actaapa.2021.8. PMID 33765756. S2CID 232366948.
- ^ a b c d McNiff JM, Subtil A, Cowper SE, Lazova R, Glusac EJ (July 2005). "Cellular digital fibromas: distinctive CD34-positive lesions that may mimic dermatofibrosarcoma protuberans". Journal of Cutaneous Pathology. 32 (6): 413–8. doi:10.1111/j.0303-6987.2005.00358.x. PMID 15953374. S2CID 12366680.
- ^ DiCicco B, Johnson W, Allred J, Soldano AC, Ramsdell WM (May 2016). "Koenen's tumor and facial angiofibromas in a case of Birt-Hogg-Dubé syndrome: A cutaneous contribution to growing evidence of a relationship with tuberous sclerosis complex". JAAD Case Reports. 2 (3): 196–8. doi:10.1016/j.jdcr.2016.03.014. PMC 4885148. PMID 27274535.
- ^ Longhurst WD, Khachemoune A (November 2015). "An unknown mass: the differential diagnosis of digit tumors". International Journal of Dermatology. 54 (11): 1214–25. doi:10.1111/ijd.12980. PMID 26235189. S2CID 5471149.
- ^ Molly Housley Smith, D.M.D. "Oral cavity & oropharynx — Soft tissue tumors & proliferations — Irritation fibroma". pathology Outlines. Topic Completed: 26 October 2020. Minor changes: 26 October 2020
- ^ Bukhari AF, Farag AM, Treister NS (October 2020). "Chronic Oral Lesions". Dermatologic Clinics. 38 (4): 451–466. doi:10.1016/j.det.2020.05.006. PMID 32892854. S2CID 221525491.
- ^ Amano R, Saruta J, Sakaguchi W, Kubota N, Fuchida S, Tsukinoki K (September 2021). "Histopathological analysis of the association between mucosal epithelial changes and the lamina propria vascular network in irritation fibroma" (PDF). Journal of Oral Biosciences. 63 (3): 278–283. doi:10.1016/j.job.2021.07.002. PMID 34280532.
- ^ Mehan R, Rupa V, Lukka VK, Ahmed M, Moses V, Shyam Kumar NK (December 2016). "Association between vascular supply, stage and tumour size of juvenile nasopharyngeal angiofibroma". European Archives of Oto-rhino-laryngology. 273 (12): 4295–4303. doi:10.1007/s00405-016-4136-9. PMID 27289235. S2CID 9509112.
- ^ Li W, Ni Y, Lu H, Hu L, Wang D (June 2019). "Current perspectives on the origin theory of juvenile nasopharyngeal angiofibroma". Discovery Medicine. 27 (150): 245–254. PMID 31421693.
- ^ a b Sbaraglia M, Bellan E, Dei Tos AP (April 2021). "The 2020 WHO Classification of Soft Tissue Tumours: news and perspectives". Pathologica. 113 (2): 70–84. doi:10.32074/1591-951X-213. PMC 8167394. PMID 33179614.
- ^ Ali Z, Anwar F (November 2019). "Angiofibroma of Soft Tissue: A Newly Described Entity; A Case Report and Review of Literature". Cureus. 11 (11): e6225. doi:10.7759/cureus.6225. PMC 6929243. PMID 31890425.
- ^ Kallen ME, Hornick JL (January 2021). "The 2020 WHO Classification: What's New in Soft Tissue Tumor Pathology?". The American Journal of Surgical Pathology. 45 (1): e1–e23. doi:10.1097/PAS.0000000000001552. PMID 32796172. S2CID 225430576.
- ^ a b Libbrecht S, Van Dorpe J, Creytens D (March 2021). "The Rapidly Expanding Group of RB1-Deleted Soft Tissue Tumors: An Updated Review". Diagnostics (Basel, Switzerland). 11 (3): 430. doi:10.3390/diagnostics11030430. PMC 8000249. PMID 33802620.
- ^ Mandato VD, Santagni S, Cavazza A, Aguzzoli L, Abrate M, La Sala GB (July 2015). "Cellular angiofibroma in women: a review of the literature". Diagnostic Pathology. 10: 114. doi:10.1186/s13000-015-0361-6. PMC 4506619. PMID 26187500.
- ^ Chapel DB, Cipriani NA, Bennett JA (January 2021). "Mesenchymal lesions of the vulva". Seminars in Diagnostic Pathology. 38 (1): 85–98. doi:10.1053/j.semdp.2020.09.003. PMID 32958293. S2CID 221842800.
- ^ a b c Paral KM, Petronic-Rosic V (2017). "Acral manifestations of soft tissue tumors". Clinics in Dermatology. 35 (1): 85–98. doi:10.1016/j.clindermatol.2016.09.012. hdl:10161/13269. PMID 27938817.