Vulvar vestibulitis syndrome (VVS), vestibulodynia, or simply vulvar vestibulitis, is vulvodynia localized to the vulvar vestibule. It tends to be associated with a highly localized "burning" or "cutting" type of pain. Until recently, "vulvar vestibulitis" was the term used for localized vulvar pain: the suffix "-itis" would normally imply inflammation, but in fact there is little evidence to support an inflammatory process in the condition. "Vestibulodynia" is the term now recognized by the International Society for the Study of Vulvovaginal Disease.[1]
Provoked vestibulodynia, pain provoked by contact localized to the vulvar vestibule, is the most common subtype of vulvodynia among premenopausal women.[2] The condition has been cited as affecting about 10% to 15% of women seeking gynecological care.[3]
Symptoms edit
Vestibulodynia is characterized by severe pain with attempted penetration of the vaginal orifice and reports of tenderness with pressure within the vulval vestibule. Usually there are no reports of pain with pressure to other surrounding areas of the vulva. The feelings of irritation and burning can persist for hours or days following sexual activity. Vestibulodynia also can often cause sex to be painful, known as dyspareunia.[3][4][5]
The pain may be provoked by touch or contact with an object, such as the insertion of a tampon, with vaginal intercourse, or with the pressure from sitting on a bicycle seat, (provoked vestibulodynia)[6] or it may be constant and not provoked by a physical stimulus (unprovoked vestibulodynia). Some women have had pain since their first penetration (primary vestibulodynia) while some have had it after a period of time with pain-free penetration (secondary vestibulodynia).
The disease may have social and psychological ramifications. Many people with vulvovaginal pain experience of chronic frustration, disappointment, hopelessness and depression because of the impacts that the disease has on their lives. It can negatively impact a person's quality of life, their romantic and sexual relationships, and their ability to participant in normal activities.[7]
Causes edit
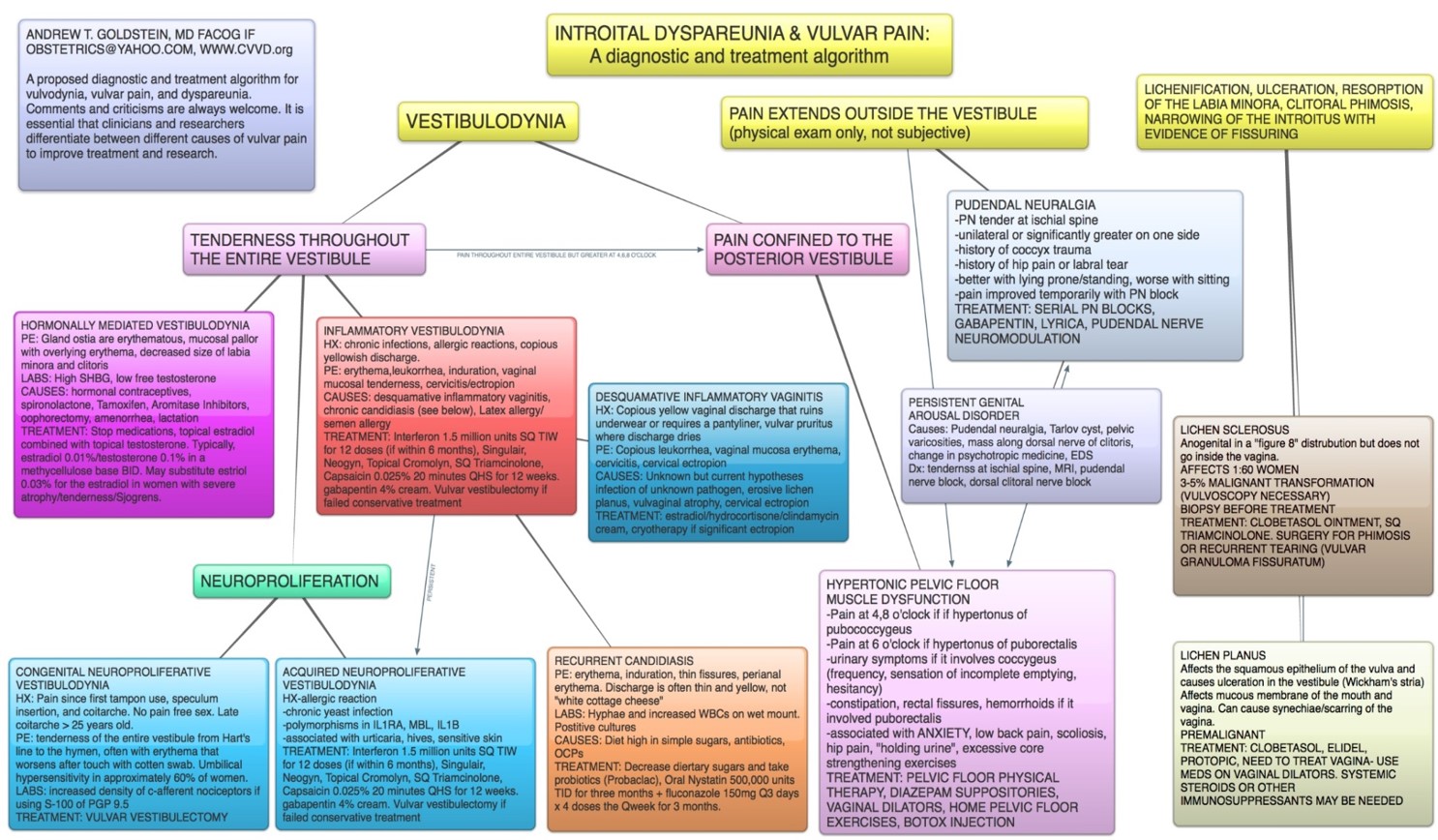
The mechanisms underlying vestibulodynia are not yet fully understood. There are thought to be several subtypes.
Neuroproliferative vestibulodynia is a disease where in there are an excess of pain receptors (C-afferent nociceptors) and mast cells in the vestibule. There can be around 10 times the normal density of these pain receptors. Some people are born with this condition (congenital neuroproliferative vestibulodynia). Many of those born with congenital neuroproliferative vestibulodynia also experience hypersensitivity in their belly-button because both the vulvar vestibule and the belly-button develop from the same tissue in embryo (primitive urogenital sinus).[8]
Others develop neuroproliferation later in life (acquired neuroproliferative vestibulodynia), perhaps as part of an immune response to infection or allergy.[8] A number of causes may be involved, including subclinical human papillomavirus infection, chronic recurrent candidiasis, or chronic recurrent bacterial vaginosis.[4][5]
Vestibulodynia can also be mediated by hormonal imbalances (hormonally-mediated vestibulodynia), and sometimes caused by hormonal contraceptives. Estrogen-based birth control has been shown to increase the risk of vestibulodynia by up to 11 times.[9] Labs may show high sex hormone binding globulin or low free testosterone.[10]
Hypertonic pelvic floor dysfunction is present in many people who have vestibulodynia. Tight muscles can even contribute to and cause pain in the posterior area of the vestibule. People with hypertonic pelvic floor dysfunction may experience urinary symptoms like urgency and/or symptoms like constipation, rectal fissures, hip pain, and/or lower back pain. [10]
Pain extending outside of the vulvar vestibule may have other sources. Damage to the pudendal nerve ("pudendal neuralgia" or pudendal nerve entrapment) can cause unilateral or bilateral pain. Persistent genital arousal disorder can also cause pain in the vulvar vestibule. Spinal pathology can also cause vulvar pain.[10]
In recent years, diagnostic algorithms for the diagnosis of the various sub-types of vulvodynia have been developed and refined.[10] The International Society for the Study of Women's Sexual Health (ISSWSH) supports this diagnostic algorithm.
{kind=link}
Diagnosis edit
For many people with vulvodynia, getting diagnosed and treated is very difficult. Getting an accurate diagnosis often takes years.[11] A 2012 survey found that less the 2% of people who sought care for symptoms of vulvar pain were able to get a diagnosis.[12]
Diagnosis is made by the q-tip cotton-swab test, in which pressure is applied in a circular fashion around the vulvar vestibule to assess complaints of pain. Laboratory tests are used to exclude bacterial, viral or yeast infection. Laboratory tests can also be used to check the patient's sex hormones to see if there may be a hormonal component. A careful examination of the vulvovaginal area is conducted to assess whether any atrophy is present.
Treatment edit
Treatment depends on the subtype of disease.
For congenital neuroproliferative vestibulodynia, the gold-standard treatment is a surgery to remove the vestibule, called vestibulectomy. Acquired neuroproliferative vestibulodynia and inflammatory vestibulodynia may be treated with topicals. When such conservative treatments fail, vestibulectomy may be an option.[10]
Hormonally-mediated vestibulodynia is treated by stopping offending medications (commonly, hormonal birth control) and applying topical estradiol combined with topical testosterone. This allows the vulvar tissue to return to a healthy state.[10]
Pelvic floor dysfunction can be treated with pelvic floor physical therapy.
Treatment typically requires a multidisciplinary team including a gynecologist, a pelvic floor physical therapist, sometimes a surgeon, and sometimes a counsellor to help patients navigate the psychosocial burdens of the condition. [13][14][15][16]
References edit
- ^ "Home". issvd.org.
- ^ Rosen, Natalie O.; Dawson, Samantha J.; Brooks, Melissa; Kellogg-Spadt, Susan (2019). "Treatment of Vulvodynia: Pharmacological and Non-Pharmacological Approaches". Drugs. 79 (5): 483–493. doi:10.1007/s40265-019-01085-1. ISSN 1179-1950. PMID 30847806. S2CID 73485304.
- ^ a b Bergeron S, Binik YM, Khalifé S, Meana M, Berkley KJ, Pagidas K (1997). "The treatment of vulvar vestibulitis syndrome: Toward a multimodal approach". Sexual and Relationship Therapy. 12 (4): 305–11. doi:10.1080/02674659708408174.
Bergeron S, Binik YM, Khalifé S, Pagidas K (1997). "Vulvar vestibulitis syndrome: a critical review". Clin J Pain. 13 (1): 27–42. doi:10.1097/00002508-199703000-00006. PMID 9084950. - ^ a b Marinoff SC, Turner ML (1991). "Vulvar vestibulitis syndrome: an overview". Am J Obstet Gynecol. 165 (4 Pt 2): 1228–33. doi:10.1016/S0002-9378(12)90732-2. PMID 1659198.
- ^ a b Peckham BM, Maki DG, Patterson JJ, Hafez GR (April 1986). "Focal vulvitis: a characteristic syndrome and cause of dyspareunia. Features, natural history, and management". Am J Obstet Gynecol. 154 (4): 855–64. doi:10.1016/0002-9378(86)90472-2. PMID 3963075.
- ^ http://www.abc.net.au/radionational/programs/healthreport/treatment-of-sexual-difficulties-and-research-into-asexuality/4058034 Suggested treatment for sexual difficulties and research into asexuality, Dr Lori Brotto, 11 June 2012, ABC Radio National
- ^ Goldstein, Andrew; Pukall, Caroline; Goldstein, Irwin (2021). Female Sexual Pain Disorders: Evaluation and Management (2 ed.). p. 143.
- ^ a b Rubin, Rachel; W., Caitlin. "Neuroproliferative Vestibulodynia". www.prosayla.com. Retrieved 29 March 2024.
- ^ Aerts, Leen; Pluchino, Nicola (13 December 2021). "Hormonal contraception and vulvodynia: an update". GREM - Gynecological and Reproductive Endocrinology & Metabolism. 2 (3/2021): 156–161. doi:10.53260/GREM.212034. ISSN 2710-2297. Retrieved 29 March 2024.
- ^ a b c d e f Goldstein, Andrew; Pukall, Caroline; Goldstein, Irwin (2021). Female Sexual Pain Disorders: Evaluation and Management (2 ed.). pp. 157–162.
- ^ Harlow, Bernard (2014). "Prevalence of Symptoms Consistent with a Diagnosis of Vulvodynia: Population-based estimates from two geographical regions". American Journal Obstetrics and Gynecology. 210 (1): 40.e1–8. doi:10.1016/j.ajog.2013.09.033. PMC 3885163. PMID 24080300.
- ^ Reed, Barbara Diane; Harlow, Siobán Denise; Sen, Ananda; Legocki, Laurie Jo; Edwards, Rayna Monique; Arato, Nora; Haefner, Hope Katharine (February 2012). "Prevalence and demographic characteristics of vulvodynia in a population-based sample". American Journal of Obstetrics and Gynecology. 206 (2): 170.e1–9. doi:10.1016/j.ajog.2011.08.012. ISSN 1097-6868. PMC 3779055. PMID 21963307.
- ^ https://www.socialstyrelsen.se/publikationer2018/2018-6-16[permanent dead link] Socialstyrelsen. Kartläggning av vestibulit: Förekomst och behandling av flickor och kvinnor med vestibulit samt behov av kunskapsstöd Sweden: Socialstyrelsen; 2018
- ^ https://www.sfog.se/natupplaga/ARG_nr%2071_webae1437d4-8cc5-4457-9eac-f5c6550a614b.pdf SFOG. Vulvovaginala sjukdomar Sweden: Elanders AB; 2013. 71
- ^ Faye RB, Piraccini E. Vulvodynia. [Updated 2020 Jan 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430792/
- ^ Goldstein, A. T., Pukall, C. F., Brown, C., Bergeron, S., Stein, A., & Kellogg-Spadt, S. (2016). Vulvodynia: Assessment and Treatment. J Sex Med, 13(4), 572-590. doi: 10.1016/j.jsxm.2016.01.020